Last updated on Jun 20, 2026
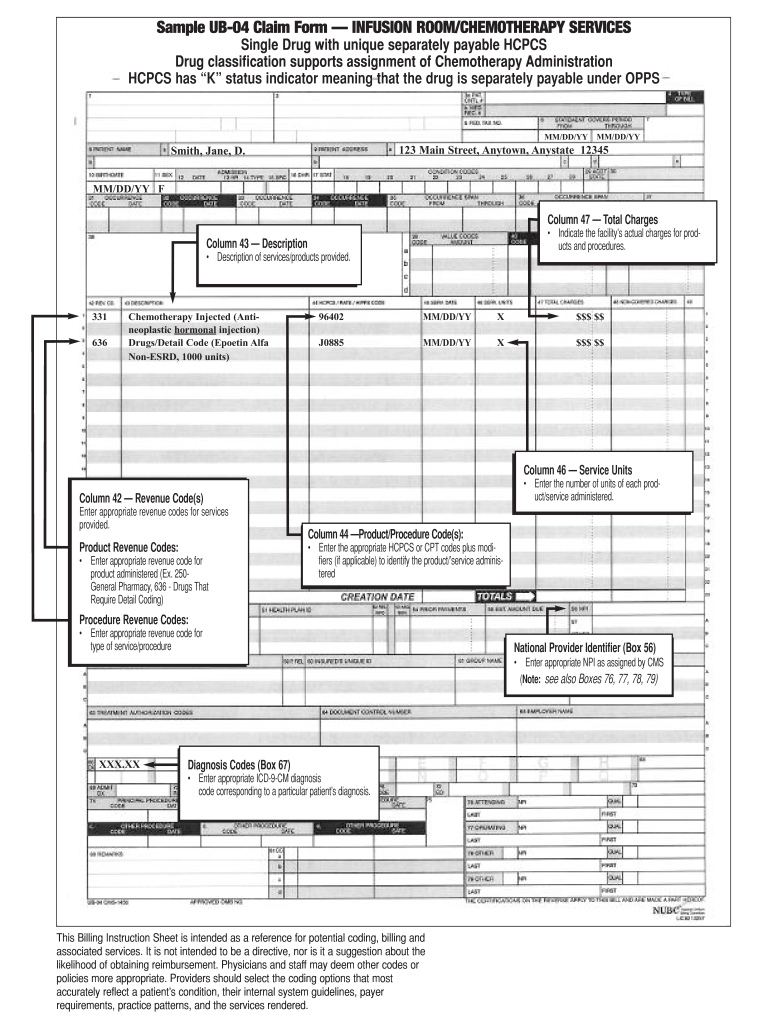
Sample UB-04 Claim Form free printable template
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Sample UB-04 Claim Form
The UB-04 Claim Form is a medical billing document used by healthcare facilities to submit claims for services rendered, including treatments like chemotherapy.
pdfFiller scores top ratings on review platforms
This product is fantastic! It has so many great features that I didn't even realize came with the subscription!
Just as easy as getting the forms straight from the courts. I love it!
Who needs Sample UB-04 Claim Form?
Explore how professionals across industries use pdfFiller.

Sample UB-04 Claim Form is needed by:
-
Healthcare providers
-
Hospitals and clinics
-
Medical billing professionals
-
Insurance companies
-
Billing administrators
-
Pharmaceutical companies
Comprehensive Guide to Sample UB-04 Claim Form
Understanding the UB-04 Claim Form
The UB-04 Claim Form is a critical component of the healthcare billing process, serving as a standardized document used by healthcare providers to request reimbursement for services rendered. This healthcare claim form primarily facilitates billing for hospital services, including essential treatments like chemotherapy and drug administration. By understanding the significance of the UB-04 claim form, healthcare facilities can ensure accurate submissions that help streamline their billing operations.
Purpose and Benefits of the UB-04 Claim Form
The UB-04 Claim Form plays a vital role in ensuring that healthcare providers receive timely reimbursement for their services. Its structured nature enables a more efficient billing process that helps reduce claim denials, thereby expediting payment cycles. By utilizing this medical billing form, healthcare organizations can not only improve their financial processes but also enhance the overall patient experience by ensuring services are billed correctly and credibly.
Key Features of the UB-04 Claim Form
-
The UB-04 form template includes numerous fields specifically designed for patient information and detailed service descriptions.
-
Accurate coding is imperative, relying on revenue codes to represent the services rendered accurately, ensuring proper billing.
-
The structured format facilitates straightforward data entry and minimizes misunderstandings in the billing process.
Who Needs to Use the UB-04 Claim Form?
This hospital billing form is essential for various healthcare facilities, including hospitals, clinics, and rehabilitation centers. Healthcare providers, particularly those involved in billing, must be familiar with this form to ensure compliance and accuracy in their reimbursement claims. Understanding who utilizes the UB-04 form contributes to more effective management of billing activities in the healthcare industry.
How to Fill Out the UB-04 Claim Form: Step-by-Step
Completing the UB-04 Claim Form accurately is crucial for successful reimbursement. Here’s a step-by-step guide:
-
Gather essential patient information such as name, address, and insurance details.
-
Detail the services provided, including treatment type and any associated revenue codes.
-
Input the charges for all services rendered and ensure they correspond with the services listed.
-
Review the form field by field to avoid common mistakes that could delay claims.
Submission Methods and Important Deadlines for the UB-04 Claim Form
When it comes to submitting the UB-04 Claim Form, healthcare providers have multiple options at their disposal. Submission can occur electronically or via mail, depending on the preferences of the facility. It's essential to be aware of the deadlines for filing claims to avoid implications that could arise from late submissions, which may lead to delayed payments or claim rejections.
Common Errors When Filing the UB-04 Claim Form and How to Avoid Them
Filing the UB-04 Claim Form comes with potential pitfalls that can hinder the reimbursement process. Common errors include:
-
Incorrect patient information, which can lead to claim denials.
-
Missing revenue codes that are necessary for accurate billing.
To minimize these errors, implement a robust review checklist system to validate information before submission, ensuring accuracy and compliance.
Security and Compliance When Using the UB-04 Claim Form
Handling patient information through the UB-04 Claim Form mandates strict adherence to security measures. This includes ensuring compliance with HIPAA regulations to protect sensitive healthcare data. Utilizing secure platforms for filling out and submitting the form adds an additional layer of security, safeguarding patient information against unauthorized access.
Using pdfFiller to Complete Your UB-04 Claim Form
pdfFiller offers a seamless solution for completing and managing the UB-04 Claim Form. Key features of pdfFiller include:
-
Easy editing capabilities to modify text and information as needed.
-
Cloud storage for secure document management and accessibility.
-
eSigning options that simplify the approval process without requiring additional software.
This user-friendly platform allows healthcare providers to fill out the form from any browser, enhancing convenience and efficiency.
Real-Life Example: Completed UB-04 Claim Form
For a better understanding of how the UB-04 Claim Form should be filled out, reviewing a sample completed UB-04 claim form can be extremely helpful. Look for key components such as accurate patient details, clearly defined service descriptions, and properly formatted charges. Familiarizing yourself with a completed form aids in ensuring compliance and facilitates accurate billing practices.
How to fill out the Sample UB-04 Claim Form
-
1.To access the UB-04 Claim Form on pdfFiller, start by navigating to the pdfFiller website and using the search bar to find "UB-04 Claim Form", then select it from the search results.
-
2.Once the form is open, click on the various fields to fill in details. Use the toolbar to add text, checkboxes, or other tools available on pdfFiller to complete the necessary sections.
-
3.Before filling out the form, gather essential patient information, including names, addresses, insurance details, and specifics about services provided to ensure accurate completion.
-
4.Carefully navigate through each section of the form. Fill in all required fields including patient demographics, service descriptions, revenue codes, and charges, ensuring accuracy throughout the process.
-
5.After completing the form, review all entered information for correctness and completeness to avoid potential submission errors.
-
6.Once satisfied with the form's contents, you can save your work directly on pdfFiller, download the completed form to your device, or submit it electronically to the appropriate insurance agency as required.
What are the eligibility requirements for using the UB-04 Claim Form?
To use the UB-04 Claim Form, healthcare facilities must be providing billable medical services, including hospital care and outpatient treatments, and must be registered with appropriate insurance providers.
What is the usual turnaround time for processing claims submitted on the UB-04 form?
Processing times for claims submitted using the UB-04 Claim Form typically vary by insurance provider but generally take between 14 to 30 days, depending on completeness and accuracy of the submission.
What supporting documents are required when submitting the UB-04 Claim Form?
Common supporting documents include patient medical records, insurance information, and any applicable consent forms. Ensure all documents are organized and accompany the claim for faster processing.
How can I submit the UB-04 Claim Form after filling it out?
You can submit the UB-04 Claim Form electronically through pdfFiller by selecting the submit option, or you may download it and submit it manually to the appropriate insurance company via mail.
What are some common mistakes to avoid when filling out the UB-04 Claim Form?
Common mistakes include incomplete fields, inaccurate coding for services, and failing to provide necessary supporting documents. Always double-check for accuracy before submission.
Are there any fees associated with using the UB-04 Claim Form?
There are typically no fees associated specifically with the UB-04 Claim Form itself, but healthcare providers may incur costs related to electronic submission services or software use.
Can I find a blank template for the UB-04 Claim Form online?
Yes, a PDF template of the UB-04 Claim Form can often be located online through healthcare resources or directly on pdfFiller for easy fillable access.
Related Content
Related Forms




Related Catalogs
Get the latest insights from our blog

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.